Pharyngitis
Quick Notes:
- Main infectious causes: Viral, Strep, EBV, Mycoplasma
- In general, antimicrobial therapy is of no proven benefit for treatment of pharyngitis due to bacteria other than GAS (with the exception of relatively rare infections caused by other bacterial pathogens such as Corynebacterium diphtheriae and Neisseria gonorrhoeae)
Viral
- majority of cases
- Some etiologies:
- enteroviruses, i.e. adenoviruses (pharyngoconjunctival fever)
- coxsackie A (herpangina (oral lesions only) - common in infants/young children, hand-foot-mouth)
- parainfluenza
- HSV usually causes stomatitis, rare pharyngitis; 10 percent have a tell-tale ulcerative lesion of the lip; may cause pharyngitis in the immunocompromised; stomatitis caused by herpes simplex usually is confined to the anterior buccal mucosa but may extend to the tonsillar pillars. In these more extensive cases, the child may complain of a sore throat.
- Fever, pain, anorexia, malaise
- Conjunctivitis, rhinitis, cough, stomatitis, diarrhea
- tonsillar exudates
- 24 hours -5 days
GABHS
- Group A Beta-hemolytic strep (Strep pyogenes); Most frequent bacterial cause
- <15% of cases in children age 5-15; in winter months during outbreaks, up to 30%
- Symptoms: usually abrupt onset HA/abd pain/Vomiting/fever, Throat pain, 1/3 with tonsillar pain, enlargement, exudates; palatal petechiae, diffuse erythema; fever for 1-4 days, symptoms usually resolve spontaneously in 3-5 days.
- Children under age 1: fussines, decreased appetite, low grade fever; often contact with strep+ person
- Children under age 3: atypical sx: protracted sx of nasal congestion/discharge; low grade fever, anterior cervical adenopathy, termed streptococcosis
- In the ER, rapid streptococcal antigen detection kits are available. They are
highly specific but lack sensitivity. Therefore, a throat culture should always
be sent when 48-hour follow-up is possible.
- Systems for diagnosis:
- Patients presenting with pharyngitis accompanied by certain findings should
be treated in the emergency department for presumed GABHS, according to Rosen
et al.
- fever exceeding 38.3°C
- pharyngeal or tonsillar exudates
- tender anterior cervical
adenopathy s
- Mengert adds lack of cough to the list of accompanied findings but recommends empiric
treatment if 2 or more of these 4 findings are present.
- In the following list, with a score of six, the likelihood of a + throat culture is approximately 85 percent. With a score of five, likelihood falls to 50 percent. Wald, ER, Green, MD, Schwartz, B, Barbadora, K. A streptococcal score card revisited. Pediatr Emerg Care 1998; 14:109.
- Age (5 to 15 years)
- Season (late fall, winter, early spring)
- Evidence of acute pharyngitis (erythema, edema, and/or exudates) on physical examination
- Tender, enlarged (>1 cm) anterior cervical lymph nodes
- Middle-grade fever (between 101 and 103ºF)
- Absence of usual signs and symptoms associated with viral upper respiratory tract infections
- Laboratory
- Suggest initial testing with a standard throat culture
- Suggest rapid strep testing only for children with a streptococcal score of ≥5 or if the results of the standard throat culture will not be available for more than 48 hours.
- Because some RADT may miss as many as 35 percent of cases of GAS pharyngitis, we recommend that throat culture be performed in children and adolescents with negative rapid strep test
- True streptococcal infection may be confirmed by measurement of antistreptococcal antibody titers (eg, antistreptolysin O, anti-deoxyribonuclease B, hyaluronidase, streptokinase, or nicotinic acid dehydrogenase).
- the antibody response occurs 2-3 weeks after infection onset; the antibody response is frequently aborted by early and appropriate antibiotic therapy
- Serologic testing for GAS may be necessary to confirm previous infection in patients who are being evaluated for ARF or PSGN.
- Carriers
- GAS resides in the oropharynx of streptococcus carriers in the absence of host immunologic response to the organism
- In temperate climates during the winter and spring up to 20 percent of asymptomatic school-aged children may be carriers.
- pharyngeal strep carriers tend to have very low ASO titers; they may be just above detectable.
- Streptococcus carriers are unlikely to spread the organism to close contacts and are at very low risk for developing suppurative complications or acute rheumatic fever
- eradication of GAS from the upper respiratory tract of carriers is much more difficult than eradication of GAS from patient with acute infections
- In general, except i.e multiple recurrent episodes, streptococcus carriers do not require antimicrobial therapy.
- Treatment:
- Fever and constitutional symptoms usually resolve within three to four days, even in the absence of antimicrobial therapy. Clinical improvement has been observed up to 48 hours sooner in patients receiving penicillin versus placebo within the first two days of illness
- Try to start antibiotic therapy within 9 days of onset of symptoms to prevent rheumatic fever (although may be less effective for prevention of suppurative complications). Do not delay treatment, if patient is severely ill or if highly virulent or rheumatogenic strains are actively circulating within a community.
- Duration of therapy 10 days. Exceptions: 5 days of cefpodoxime, cefdinie or azithro.
- single-dose benzathine penicillin
G IM, or 10 days of PO penicillin.
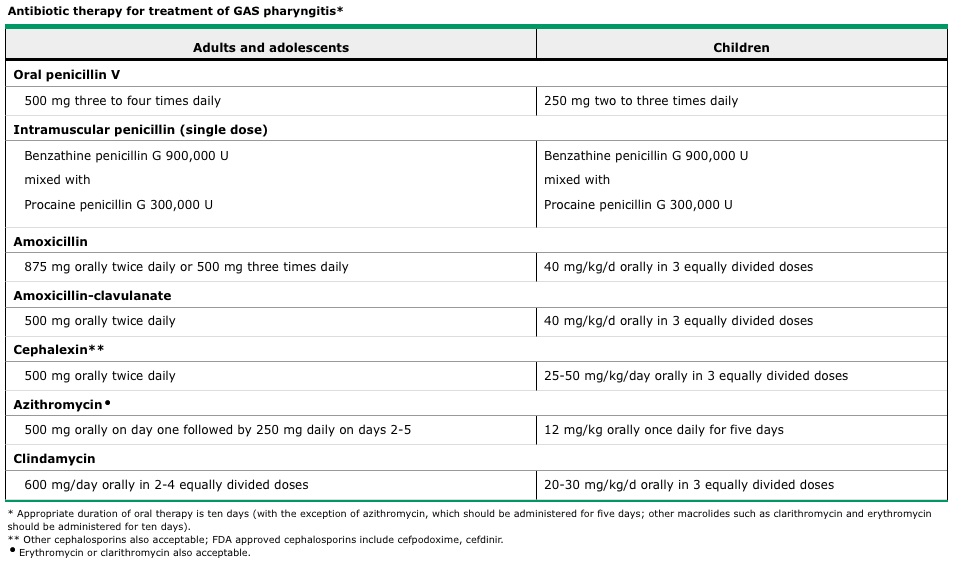
- Sulfonamides and tetracyclines should not be used d/t high rates of resistance to these agents and their frequent failure to eradicate even susceptible organisms from the pharynx.
- Amoxicillin-clavulanate may be useful in patients with recurrent GAS infection
- Cephalosporins have demonstrated better microbiologic and clinical cure rates than penicillin; these differences appear to be greater among children than adults, and some favor use of first generation cephalosporins as first line therapy in this group. But, (1) more expensive (2) may facilitate development of antibiotic resistance
- Beta-lactam hypersensitivity:
- cephalosporins (cefuroxime, cefpodoxime, cefdinir, and ceftriaxone) may be used, in the absence of history of life threatening allergic reaction
- Macrolides (clarithromycin, azithromycin or erythromycin) are an acceptable alternative for penicillin allergic patients, depending on local resistance patterns
- For the rare patient with an erythromycin-resistant strain of GAS who is unable to tolerate beta lactam agents, clindamycin is an appropriate choice.
Infectious Mononucleosis (Epstein-Barr Virus/CMV)
- Most commonly in adolescents
- **don't miss** teens with mononucleosis-like syndrome: test for HIV.
Mycoplasma pneumoniae
- can cause pharyngitis in children older than 6 years.
- accounts for 5 to 16 percent of cases of pharyngitis (with the variability possibly attributable to the cyclic nature of infections caused by M. pneumoniae)
Be aware of the differential diagnosis:
- epiglottitis: toxic appearance, high fever, stridor, drooling, unimmunized. Sore throat is rarely the primary complaint
- retropharyngeal abscess: sore throat, usually under age 4, neck pain, fever, dysphagia, maybe respiratory distress; posterior location makes visualization difficult
- lateral pharyngeal abscesses: similar sx to retropharyngeal, but less often. High fever, trismus, swelling below the mandible
- peritonsillar abscess: may be a superinfection; bulge in posterior aspect of soft palate; deviates uvula; fluctuant
- infectious mononucleosis: rare airway obstruction from severe tonsillar hypertrophy
- diphtheria (Corynebacterium diphtheriae): thick pharyngeal membrane and marked cervical adenopathy
- Lemierre's syndrome: unusual mixed anaerobic infection is associated with jugular venous thrombophlebitis and the dissemination of infection by septic emboli. It should be considered in the ill-appearing patient with severe pharyngitis
Other unusual causes
- Neisseria gonorrhea, oropharyngeal tularemia (where endemic; should be considered in patients with pharyngitis that is unresponsive to penicillin and a history of ingestion of poorly cooked meat from wild animals or contaminated water)
- Implicated as agents: Group C and G strep, Arcanobacterium hemolyticum (clinical features overlap with GAS incl scarlatiniform rash on extensor surfaces of arms - unresp to PCN; use erythro) and Chlamydia pneumoniae
CHLA Board Review 2005
Rosen P: Group A beta-hemolytic streptococcal pharyngitis.
In: Rosen P, ed. Emergency Medicine. 2nd ed. St. Louis: Mosby-Year Book; 1992.
Mengert TJ: Pharyngitis. In: Emergency Medical Therapy. 4th ed. Philadelpha: WB
Saunders; 1996: 480.UpToDate.com: Evaluation of sore throat in children. Update: June 9, 2008.